
Overview

Contact
What Is ACL Reconstruction Surgery?
ACL reconstruction is a cutting-edge, minimally invasive arthroscopic surgery designed to repair a torn anterior cruciate ligament – the critical knee stabilizer essential for pivoting, twisting, and high-impact activities. Often resulting from sports injuries in soccer, basketball, hockey, skiing, or everyday accidents, an ACL tear can cause debilitating symptoms like knee “giving way,” persistent swelling, pain, and limited mobility. If left untreated, it heightens risks of chronic instability, secondary injuries (e.g., meniscus or cartilage damage), and early-onset osteoarthritis.
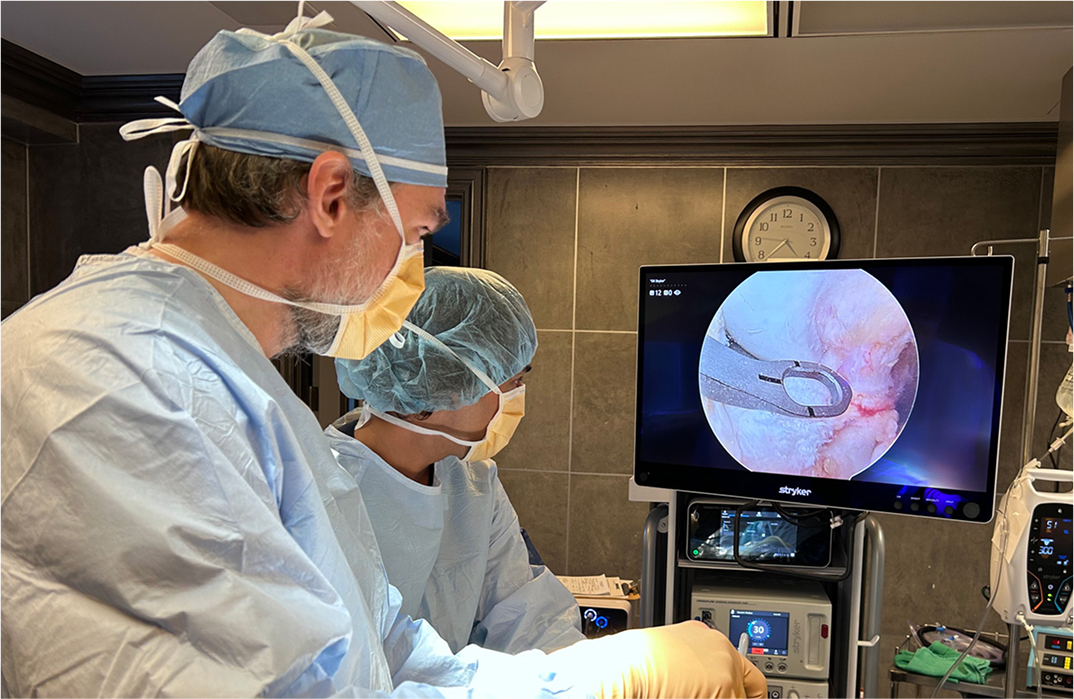
At OV Surgical, we elevate ACL surgery in Canada with advanced techniques that minimize downtime and maximize results. Through just two tiny incisions (less than 1 cm), our surgeons insert an arthroscope – a small camera – to visualize and address associated knee issues in real-time. Following diagnostic arthroscopy, we make an incision to obtain a graft that will used to recreate the ACL in your knee. To reconstruct the ACL, we prioritize autografts harvested from your own body, such as the patellar tendon, quadriceps tendon, or hamstring tendon, for optimal strength and biomechanical function. Once the knee has been prepared and the ACL graft has been appropriately positioned in the knee, the graft is meticulously secured to the femur and tibia using strong fixation methods.
In high-risk cases involving severe instability, hyperextension, or revisions, we may incorporate a lateral extra-articular tenodesis (LET) for enhanced rotational control. In this case, a small strip of the iliotibial (IT) band is used to perform the LET augmentation procedure.
Recovery
Post-procedure, our evidence-based protocols integrate cryotherapy, neuromuscular electrical stimulation (NMES), and progressive physiotherapy to accelerate healing and restore your function. With respect to early mobility, expect to ambulate with crutches within 1-3 days and start targeted physiotherapy within the first week. Our customized rehab plans, crafted in collaboration with leading physiotherapists, aim for full motion by 6-8 weeks and strength milestones by 6 months. Most patients achieve sports clearance in 6-9 months, verified through rigorous testing like quadriceps strength assessments (>90% symmetry), single-leg hops, and stability evaluations. We emphasize psychological readiness too, ensuring you’re mentally prepared for high-level performance.


Benefits
With success rates of 90-95%, private ACL reconstruction at OV Surgical restores knee stability, prevents re-injury, allows you to get back to the sports and/or other aspects of life that are important to you. Our patients report enhanced knee function, confidence, and quality of life, backed by meticulous follow-up and data-driven protocols.
FAQ
Contact
